

A staff member of the German Ebola Treatment Unit in Monrovia in February 2015.
Photo: C. Janke
 Download this article in magazine layout
Download this article in magazine layout
- Share this article
- Subscribe to our newsletter
Between ignorance, misperception and dilemma
In clinical medicine, the term “crisis” tends to be perceived differently from its colloquial use. Here, it lacks the almost exclusively negative, apocalyptic connotation it bears in everyday language. Instead, the high development potential during a crisis is recognised, and the probability of attaining a new equilibrium as a result is understood both as a risk and an opportunity. Given the 11,299 deaths (status: 08.11.15), the disrupted families, the suffering of the survivors, the many orphans, the compromised health system and the medium- to long-term psychological, economic and political consequences of the Ebola outbreak in West Africa, which is not over yet, it above all appears to be a disaster the impact of which has still not been fully comprehended and hence a crisis, in the conventional sense of the term, that rumbles on. Why did international support take so long to come, and why was it performed so cumbersomely and hesitantly? Why did an outbreak of such magnitude hit almost everyone involved in an unprepared state? Why were the scarce resources allocated with so little thought given to actual needs for such a long time? Why was common sense, rationality, frequently the first or at least the second victim of the outbreak? Answering these questions above all requires an analysis of misguided perceptions, assumptions and models. This article sets out from German humanitarian emergency relief in Liberia during the outbreak of Ebola in 2014/15, and thus from the lessons learnt in a close call that the German relief mission encountered within the crisis itself. For by the time the Ebola Treatment Unit (ETU) of the German Red Cross (DRK) and Federal Army Joint Support Mission was officially opened at the SKD Stadium in Monrovia on the 23rd December 2014, three months had already gone by since the mission had been assigned by the German Defence Minister. There are reasons for this time requirement. But none of them put the fact into perspective that taking three months to make an “emergency response operation” operational is wholly unacceptable and far too long. At any rate, on the day the ETU was opened, 1,440 ETU beds were available in Liberia, but, fortunately, there were now only 66 Ebola patients. The mission was about to be operationally terminated even before it had properly started working.
“Essentially, all models are wrong, but some are useful”
1,440 ETU beds for 66 Ebola patients? In a country whose health sector lacks just about everything? Obviously, in a particular field of outbreak management, what is known as case management, massive overcapacities had developed that were not corrected. But how could this have happened? As a rule, decision-making under uncertainty is based on explicit model assumptions. Not only were decisions concerning the distribution of scarce resources taken on the basis of these models, but cross-border traffic and, in some cases, even people’s civil rights were restricted. A model published by the Centers for Disease Control and Prevention of the US Department of Health & Human Services in September 2014 forecast 1.4 million incidents of Ebola in Liberia and Sierra Leone for mid-January 2015 as an extreme case and a doubling of cases every 15 to 20 days (Meltzer M. I., 2014). In retrospect, it is known that no such horror scenario occurred. Should the inadequate models now be blamed for the failures in allocation? Is the attempt to mathematically establish and forecast such complex developments a vain effort in any case?
It is true that the vast majority of models did not do justice to the complexity of events. For example, the epidemiologists underestimated the distinct effect of behavioural adaptation among key groups of the population (burial rites, no-touch policy). Perhaps an anthropologist should have helped the epidemiologists with modelling. What makes things even more complicated is that, as a rule, attempts at modelling take place far away from the epicentre, at universities in the Western world, which means that immediate “situational awareness” of outbreak events goes lost. Even so, effective outbreak management is inconceivable without suitable epidemiological models. The methods required for this purpose and specialist know-how in the areas concerned are scattered among a wide range of subject fields. Here, innovative field epidemiologists without reservations towards other fields of science concerned are needed.
The obviously uncritical adoption of the models by the decision-makers or their reluctance to adequately and immediately respond to clear discrepancies between theory and practice was at least just as problematic. Other NGOs and GOs in the immediate vicinity of the still incomplete German facilities commenced operation although the numbers of incidents were successively dropping. Whereas the dynamics of events would have necessitated a daily review of one’s own options to act, the “inertia of masses” as well as a partly inflexible central steering of Germany’s relief mission resulted in a delay of the required adaptive efforts. But by New Year’s Eve 2014 at the latest, as things stood, and following talks with national and international co-ordinators of Liberian outbreak management, it had become unequivocally clear that in its classical configuration, Germany’s Ebola Treatment Unit was not going to admit a single patient.
Disaster ethics between ignorance and dilemma
What would be even worse for a relief mission than its mere irrelevance would be violate the principle to “do not harm”, the “primum non nocere” of medical ethics. Just how easily one can fail to meet this requirement becomes apparent if one sets out from two relatively self-evident premises. First, Ebola patients ought to be treated in an isolation treatment unit. Second, non-Ebola patients should not be treated in such a unit. The illustration below shows the standardised layout of an isolation treatment unit. This is the configuration that was also used during the latest outbreak in Guinea, Sierra Leone and Liberia.
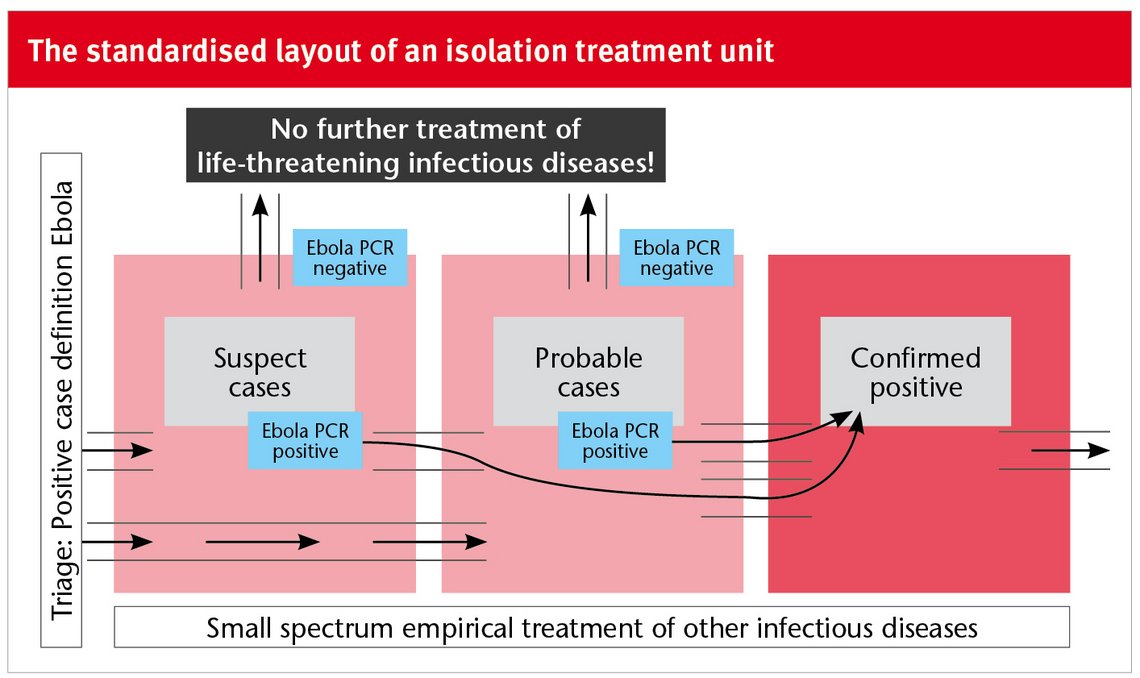
An isolation treatment unit of this kind provides neither for individual nor for sex-specific isolation. Suspected cases are initially merely allocated either to the “Suspect Cases Area” or the “Probable Case Area”, depending on their assumed risk of infection. As soon as the infection is confirmed via molecular biology virus identification, patients are transferred to the “Confirmed Positives Area”. In each of these areas, the non-Ebola patient bears a relevant, albeit differently high risk of coming into contact with the virus and becoming infected within the treatment unit. In September and October 2014, when most of the international organisations were intensifying their relief activities in West Africa, and Germany’s humanitarian mission was conducting its first explorative exercise in Monrovia, one was precisely at the apex of the outbreak curve. At this stage, a suspected case showing fever and other symptoms giving rise to suspecting Ebola (in accordance with the WHO case definition) in an ETU bore a high probability of really being infected. Up to nine out of ten suspected patients were subsequently confirmed by laboratory analysis; so, conversely, one out of every ten patients was in the wrong treatment unit – in other words, in one of the most dangerous places in the world. The only acceptable justification for this is the crisis situation itself with its blatant lack of all necessary medical resources.
By January 2015, the incidence of the disease in Liberia had dropped radically. But as a result, nine non-Ebola patients were now among the ten suspected patients admitted to the ETUs. The Ebola case definition adopted by the WHO circumscribes a complex of symptoms that occurs with a high probability when the disease is contracted. However, the probability of a symptom (or a symptom complex) occurring in Ebola is not identical with the probability of a patient showing this symptom complex having contracted Ebola. In the three countries most strongly affected, this meant that the overwhelming majority of the patients in the ETUs were now suffering from other diseases while being at risk for an Ebola virus infection in the treatment units. It therefore became more and more irrational for a patient with symptoms typical of Ebola to consult an ETU. Large numbers of suspected patients fled Monrovia, and the epidemiological need to isolate, if possible, all suspected patients was severely compromised. Outbreak management in the field of Ebola case management was now in crisis itself.
During the first few days of 2015, the officials of the German isolation unit in Monrovia, the planning of which had obviously missed the mark, sought to devise a strategy for their excellently trained and highly motivated Liberian and German specialists and for their sophisticated isolation treatment unit after all. Now, internally, the issue of comprehensively optimising Ebola case management was considered for the first time. No longer were suspected patients to be separated merely corresponding to their risk of infection, but at the same time according to the probability of their chance of not being infected. In addition to the three Suspect, Probable and Confirmed Positives Areas described above, two further separate isolation areas, an Unlikely Cases Area and a Confirmed Negatives Area were required. But since there was an abundance of conventional ETUs in the immediate vicinity of the German one, the German relief mission was able to concentrate on the complementary share, which consisted of merely three isolation areas – a Suspect Cases Area (already existent), an Unlikely Cases Area and a Confirmed Negatives Area.

The ultimate objective was to avoid Ebola infections within the treatment unit at all costs. This is why the patients’ freedom of movement in the Suspect Cases Area was confined to the space of the approx. 2 x 3 m individual treatment compartment for the short period up to the submission of the first laboratory result (4 to 12hs). Patients testing Ebola-positive were transferred to a conventional ETU, while those with negative results were immediately brought to the separate Unlikely Cases Area. Although an Ebola infection was not ruled out with absolute certainty with these patients, the risk of infectiousness for fellow patients was already approaching zero. Seventy-two hours after admission, with a negative lab result, Ebola could be ruled out with certainty, and transfer to the Confirmed Negatives Area was authorised. Here, the world now changed for the patients and those treating them. Much more time could be devoted to the individual patients, since staff no longer had to work in full protective gear. But above all, it was now possible to diagnose other diseases and offer causal treatment as well. This new type of Ebola isolation facility was referred to as a “Severe Infection Temporary Treatment Unit” (SITTU). Relatively straightforward adjustments in terms of infrastructure and procedural organisation effectively warded off a serious ethical and epidemiological problem.
From sympathetic introspections to affect heuristics
In the course of efforts to learn from the many shortcomings, wrong decisions and close calls in Ebola outbreak management, it has become clear that the “pathophysiology” cannot really be comprehended in its entirety if the phenomenon of “anxiety” is not addressed as an irrationality factor. In its largely unreflective and stymying variant of “German angst”, it affected all levels of decision-making and considerably hampered effective outbreak management.
In this sense, in addition to the fact that it would have been epidemiologically ineffective and given a corresponding ethical appraisal, the option of forming a military cordon around the entire region affected in West Africa, a gigantic “cordon sanitaire” which was accepted as a map exercise, also reflected helplessness and anxiety among the decision-makers that was only difficult to conceal by doing things merely for the sake of doing things. The same applies to the West Point disaster. In the wake of rioting and looting of an Ebola treatment unit, the Liberian government decided on the 19th September 2014 to cordon off this township in the capital and prescribe a mass quarantine for its 75,000 inhabitants that was maintained with the aid of firearms for eleven days. All these measures can only be understood when patterns going beyond pure rationality are used to explain them. By no means was this an African phenomenon. On the contrary, it was apparently possible for the factor of “angst” to emancipate itself more and more from the true risk it related to the further away one was from the epicentre. German marines operating in “Ebola Full Personal Protective Equipment” in the context of their refugee mission in the Mediterranean mission are just as much of an example of this phenomenon as is a policeman belonging to the German Ebola relief mission in Liberia who was officially forbidden to enter any public building in his Federal State in Germany for 21 days after his return from the mission. As soon as one focuses on the irrationalities of Ebola outbreak management, it becomes clear that beyond “German angst”, further psychological factors must have played a significant role. Obviously, there is a huge gap between evidence and policy in this context.
For instance, from this angle, having another look at the issue of why it took so long for Western countries to show any response, despite reports of thousands of infected persons and given a steeply rising epidemiological curve, the treatise by Professor of Psychology Paul Slovic on Mother Theresa’s “If I look at mass, I will never act…” offers a useful explanation. Other insights given by “affect heuristics”, such as the apparent need for decision-makers to achieve zero risk at almost any cost, the zero risk bias, would also provide a credible explanation of many a seemingly incomprehensible Ebola management strategy
One example here is the refitting of a German Airbus, which cost ten million euros. The Airbus was meant to ferry Ebola patients in need of intensive care during the flight. Without commenting on the probability of such a patient surviving, it has to be noted that this Airbus was again completely restored to its original condition after precisely zero mission flights. Only in a world with an abundance of resources would one not have to check such a constellation for the above-mentioned irrationality factors.
Lessons learnt?
None of the phenomena described here can be fully eliminated from crisis management, even if the underlying mechanisms are largely known. What remains is the above-mentioned gap between evidence and policy, or theory and practice. The global crises of the 21st century are characterised by an unprecedented complexity, proximity and dynamics, and in this regard, the 2014/15 Ebola outbreak in West Africa was certainly not an exception. Even though insights and analyses exist, we have every reason for concern that on the next occasion, we will again stumble over the tripwires described and analysed above.
“What if an outbreak occurs in a devastated Central African country where there is no local healthcare? What if the security situation were so bad that we could not send in international experts to advise and assist in containing the outbreak? What if infected people start to flee into cities, to neighbouring countries and eventually out of the region?”
Gro Harlem Brundtland, Norway’s former Prime Minister and Secretary-General of the WHO in “International health emergencies in failed states” in 2013
Giving more attention to Global Health Security
When the World Health Organisation (WHO) declared a “public health emergency of international concern” in August 2014 in view of the regionally unchecked spread of Ebola, this came as no surprise internationally. What was indeed far more spectacular was the UN Security Council’s declaration of the 18.09.2014 referring to the outbreak as a “threat to peace”, urging the UN member states to take swift and determined action. This request initially went unheeded and had no major consequences. Up to today, many global security players, including NATO, have not deemed any significant operative activities necessary. In Germany, too, following the UNSC declaration, it took another month for the Minister of Defence to decide to launch a Federal Army military support mission on the 23.09.2014: in a subsidiary capacity as the junior partner of the German Red Cross (DRK) and, in the absence of a correspondingly trained and equipped army corps, supported by a volunteer contingent. Since then, queries about the role of the armed forces in an outbreak of viral haemorrhagic fever have never really silenced. Even NGOs, which are traditionally wary of co-operating with the armed forces, ostentatiously and urgently called for the involvement of the military in this concrete case. Whereas the fact that conflicts create a health emergency situation has already been described by politicians such as Gro Harlem Brundtland, the UN Security Council focused on the opposite causal chain of events: a severely compromised health system becoming a “threat for peace”. Both perspectives can be substantiated with a wealth of evidence and precedence, constituting the field of Global Health Security. Thus health topics are stripped of their seemingly “soft” image and increasingly shift into the security context, where more attention and more resources are traditionally available. “Health in all policies” would be the next logical step. And to avoid any misunderstandings here, conventional armed forces really are only supposed to provide subsidiary support. “Security forces” with the ability to globally support professional outbreak management by no means have to be armed forces. With its initiative for a civil “white helmet” corps, the German Federal Government has embarked on an interesting, innovative and hopefully supranational approach.
Christian Janke, MD MPH
Lieutenant Colonel (Medical Corps)
Munich, Germany
c-janke@web.de
References and further reading
Meltzer, M.I.: Estimating the Future Number of Cases in the Ebola Epidemic – Liberia and Sierra Leone, 2014-2015. CDC. MMWR: Vol. 63 Early Release 23.09.14
Slovic, Paul: Judgment and Decision Making, vol. 2, no. 2, April 2007, pp. 79-95
News Comments
Current Print Issue


Add a comment
Be the First to Comment